Today, with one day left for people to sign up before the January 15th deadline, the Seattle Times reports that WA's tally is up to 234,000:
Washington state is on pace to increase the number of people with health insurance despite efforts by the Republican Congress and the Trump administration to gut the laws known as Obamacare that expanded insurance coverage across the nation.
*UPDATE: Some have accused me of hyperbole in the headline because a) it's a "state-approved health or financial literacy" course, not a "can you read" test and b) because it would only be required if they're unable to meet the requirements in other ways. I guess I can see their point, but it strikes me as splitting hairs:
First, "literacy course" was their wording, not mine (I guess there's a distinction between "completeing a course" and "passing a test"?).
Second, there doesn't appear to be any real description of the "courses" in question--how long it is, what the criteria for measuring "completion" is, who would be conducting the course, whether you'd have to attend classes in person (vs doing so online?), how many sessions there'd be and so forth. Here's the description as laid out in the waiver request itself:
...After trying — and failing — to get a high-profile lawsuit dismissed, Dave & Buster’s agreed to pay $7.425 million to settle the suit, which accused the restaurant and entertainment chain of illegally cutting staffers’ hours to prevent them from receiving healthcare benefits.
...As HR Morning covered previously, the ERISA lawsuit was the first case in which an employer was accused of intentionally interfering with employees’ hours to avoid the ACA’s employer mandate.
The lawsuit hinged on a very specific section of ERISA — the employees sued under ERISA Section 510.
Granted, ERISA was written primarily to apply to retirement plans. But Section 510 can be applied to a number of benefit plans as well — including healthcare coverage.
Section 510 says (the critical parts are in bold):
Whenever I write or talk about the 3-Legged Stool of the ACA and the actual flaws in the law (as opposed to the ones deliberately created by the GOP), I usually focus on two "gaps" in the legs: The APTC subsidies getting cut off at 400% FPL and being too stingy below that level, and the individual mandate not being large enough (and not being properly enforced). As it happens, part of the first problem has already been unintentionally "solved" thanks to Trump's ham-handed CSR reimbursement cut-off (which ended up increasing APTC tax credits for those below the 400% cut-off), while the second problem has just been made a whole lot worse thanks ot the GOP repealing the mandate altogether.
However, in focusing on the legs of the stool, I often forget to mention another important issue: The width of the seat itself. That is, how wide the network of doctors and hospitals which accept the policy is. The Affordable Care Act does give some guidelines/regulations about how wide ACA-compliant policy networks have to be, like so:
Of all the state-based exchanges, the one in DC has gone the longest without a formal enrollment update; the last one only included data through December 5th, a whopping 5 weeks ago. Fortunately, the DC board of directors held their monthly meeting last night and produced the following update.
As shown, the tally as of 1/8/18 is 21,352 QHP selections, slightly below last year's 21,437 as of the same date. Since DC (along with California and New York) are sticking with the full 3-month Open Enrollment Period, it should provide a good apples-to-apples comparison (and the fact that very few DC enrollees have CSR assistance also means there's a nominal CSR loading impact, either).
The final, official DC ACA exchange tally last year was 21,248, so technically speaking they've already surpassed that figure...but again, it was 21,437 as of 1/8/17, which means there were at least a few hundred people who were dropped off at the tail end due to cancelling or non-payment of their first premium.
Last week the Congressional Budget Office reported that funding the CHIP program for 5 years, which they had previously estimated would increase the federal deficit by about $8 billion over the next decade, would instead only increase it by about 1/10th as much: Roughly $800 million, a rounding error when it comes to the federal budget. The reason for this isn't that funding CHIP had suddenly become less expensive, it was instead, ironically, because due to the GOP repealing the ACA's individual mandate starting in 2019, NOT funding CHIP has suddenly become more expensive.
CMS announces new policy guidance for states to test community engagement for able-bodied adults
Will support states helping Medicaid beneficiaries improve well-being and achieve self-sufficiency
CMS today announced new guidance that will support state efforts to improve Medicaid enrollee health outcomes by incentivizing community engagement among able-bodied, working-age Medicaid beneficiaries. The policy responds to numerous state requests to test programs through Medicaid demonstration projects under which work or participation in other community engagement activities – including skills training, education, job search, volunteering or caregiving – would be a condition for Medicaid eligibility for able-bodied, working-age adults. This would exclude individuals eligible for Medicaid due to a disability, elderly beneficiaries, children, and pregnant women.
In other words, work requirements for Medicaid expansion enrollees are now officially on the table.
Early last year as an Obamacare repeal bill was flailing in the House, top Trump administration officials showed select House conservatives a secret road map of how they planned to gut the health law using executive authority.
The March 23 document, which had not been public until now, reveals that while the effort to scrap Obamacare often looked chaotic, top officials had actually developed an elaborate plan to undermine the law — regardless of whether Congress repealed it.
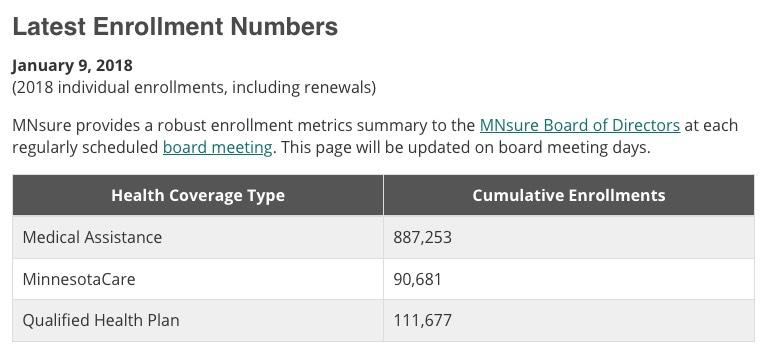
111,667 QHP selections bumps them up another 1,667, with 5 days left to go for Minnesota residents to #GetCovered for 2018. It's worth noting that enrollment in MinnesotaCare, MN's name for the ACA's Basic Health Program, has actually dropped slightly since the last hard number update I confirmed back in mid-November (93,049).
Michael Bertaut is a conservative healthcare economist in Louisiana. He and I disagree on most political issues, and he's obviously not a fan of the ACA, but he seems to be intellectually honest about his positions, and he and I have found some common ground over ACA-related stuff in the past.
Case in point: The individual mandate. Bertaut may not care for the ACA overall, but he does recognize, as I do, that if you're going to utilize the "3-legged stool" model for individual market enrollment, it has to include both a positive and negative inducement to encourage (or goad) people into enrolling...aka the Carrot and the Stick. More to the point, if you're going to have a Stick (i.e., the Individual Mandate), it has to be large enough and well-enforced enough to be effective.